A 17-day-old African boy is brought to an emergency department (ED) in his local area in respiratory distress. For the past 7 days, he has had a nonproductive cough, tactile fevers, rapid breathing, and poor feeding. The parents also note that on 2 occasions when he was short of breath, the patient’s lips and fingers turned blue. These episodes lasted less than 30 seconds, were self-resolving, and were not associated with any loss of consciousness. He has not previously seen a doctor. The parents state that they have brought the child to the ED because he seems to be worsening; the second episode in which the patient turned blue occurred earlier today. He is not taking any medications and does not have any known drug allergies. Both parents work as farmers in eastern Africa. He has 4 older siblings, all without any known medical conditions. The patient was born full-term and was delivered vaginally at home, without any complications. His birth size of 19.3 inches (49 cm) and weight of 6.4 lb (2.9 kg) are normal. Of note, the patient received minimal prenatal care.
On physical examination, the patient is awake, alert, reactive, and appears to be well-nourished. He is, however, notably pale and in obvious respiratory distress. His vital signs show a temperature of 99.5°F (37.5°C), a heart rate of 160 bpm, a respiratory rate of 56 breaths/min, a blood pressure of 87/55 mm Hg, and an oxygen saturation of 87% while breathing room air. The anterior fontanelle is normal to palpation, and no congenital abnormalities are noted on inspection of the face and head. The neck is short, the trachea is in the central position, and no jugular vein distention is appreciated. No masses, enlarged lymph nodes, or congenital defects are seen. The patient’s respiratory movements are rapid, with intercostal and subxiphoidal retractions. The heart sounds are strong, with a regular rate and rhythm and no audible murmur. The left hemithorax is clear to auscultation, without rales or wheezes; however, decreased air entry, dullness to percussion, and diffuse rhonchi are noted in the right side. The abdomen is scaphoid, soft, and nontender, with positive bowel sounds. No masses are palpated. The external genitalia appear normal for the patient’s age and gender. The extremities show good range of motion, with a capillary refill of 3 seconds. No other abnormalities are detected on the physical examination.
A complete blood cell (CBC) count reveals 13.0 ×103/µL leukocytes (13.0 × 109/L, with 45% neutrophils [0.45], 42% lymphocytes [0.42], 3% eosinophils [0.03], and no bands). No blood gas analysis is available. A chest radiograph is performed (see Figure 1). A follow-up upper gastrointestinal contrast study is also performed (see Figure 2). During the fluoroscopic evaluation, the right hemidiaphragm appears motionless.
 |
Figure 1. Lateral chest film. The lateral chest radiograph shows a diaphragm elevated more than 2 intercostal spaces over the normal side. Bowel loops are seen up into the chest. (Click to enlarge) |
 |
Figure 2. UGI contrast study. An upper gastrointestinal contrast study confirming the presence of small bowel loops in the right chest, with the diaphragm visible in the upper third of the hemithorax. (Click to enlarge) |
While still in the ED, the patient is intubated for his respiratory distress and intravenous fluids are started. He is then admitted to the neonatal intensive care unit (ICU), where he is placed in an incubator. An orogastric tube and a urine catheter are passed, and broad coverage antibiotics are started.
What is the reason for this neonate’s respiratory distress?
Discussion
|
Figure 1. Lateral chest film. The lateral chest radiograph shows a diaphragm elevated more than 2 intercostal spaces over the normal side. Bowel loops are seen up into the chest. (Click to enlarge) |
|
Figure 2. UGI contrast study. An upper gastrointestinal contrast study confirming the presence of small bowel loops in the right chest, with the diaphragm visible in the upper third of the hemithorax. (Click to enlarge) |
Diaphragmatic eventration results from underdevelopment and thinning of the central portion of one of the hemidiaphragms,[2] thereby causing a chronically elevated resting position. Diaphragmatic eventration may be congenital or acquired secondary to a phrenic nerve injury.[3] Unlike a diaphragmatic hernia, in which there is a physical breach of the diaphragm and abdominal contents may herniate into the thorax, the thorax and the peritoneum remain separated in diaphragmatic eventration.[2] Aplasia of the diaphragmatic muscle in diaphragmatic eventration may result in an elevated position of all or part of the diaphragmatic muscle. The diagnosis should be suspected when bowel sounds are auscultated in the thorax of a newborn; it is confirmed with radiologic studies.[5]
The classic clinical findings of diaphragmatic eventration include respiratory distress, cyanosis, tachypnea, and diminished breath sounds. A scaphoid abdomen should also direct the clinician’s attention toward this entity, since abdominal contents rise into the chest. Congenital diaphragmatic eventration may be apparent at birth, but delayed presentations may also occur. Patients may present with wheezing, recurrent respiratory infections (pneumonia, bronchitis, or bronchiectasis), and/or exercise intolerance (dyspnea during feeding); however, even large eventrations might be completely asymptomatic. Prominence of the ipsilateral chest and cardiac apical beat under the sternum or displaced to the opposite side (mediastinal shift) are also frequent findings.[3]
The chest radiograph is the initial study of choice. Front and lateral films will show an abnormally elevated diaphragm. In the absence of disease, the line formed by the diaphragm on chest radiography is continuous. When the diaphragm cannot be fully visualized, a pathologic condition (such as diaphragmatic eventration or, possibly, other conditions) may still exist in the appropriate clinical presentation. The affected side of the diaphragm should be at least 2 intercostal spaces higher than the normal side. Another typical finding is the presence of bowel loops in the affected thorax. A blood gas analysis may reveal respiratory acidosis. The usual confirmatory study is an upper gastrointestinal series, which will demonstrate the presence of bowel loops in the chest. Computed tomography (CT) scanning and magnetic resonance imaging (MRI) can also demonstrate this finding. The gold standard for making the diagnosis of diaphragmatic eventration, however, is confirmation of a motionless or paradoxically moving hemidiaphragm,[5] which can be done with fluoroscopy or with real-time ultrasonography. Additionally, ultrasonography does not expose the patient to ionizing radiation.
Diaphragmatic eventration may be congenital or acquired. Congenital diaphragmatic eventration is less common than the acquired variety, and it refers to a thinned central portion of the diaphragm on the affected side. It appears to be secondary to the lack of proper development of or cell migration from the four elements forming this structure, which are the septum transversum, the pleuroperitoneal folds, the body wall, and the dorsal root of the mesentery. (The phrase “Several Parts Build the Diaphragm” may be used to remember the different parts of the diaphragm.) The exact etiology of the abnormality is unknown, although it may be associated with fetal rubella or cytomegalovirus infection. There is no known familial predisposition. The acquired form, which may be clinically indistinguishable from the congenital form, is usually the result of trauma. When seen in newborns, it is secondary to birth trauma (generally, from damage to the phrenic nerve); this may be caused by excessive traction to the arm during delivery. The diaphragm eventually becomes atrophic secondary to the phrenic nerve injury and disuse, and it may eventually develop an eventration. The phrenic nerve is formed by the roots of the cervical motor neurons C3, C4, and C5 in the neck. (The phrase “C3, C4, and C5 keep the diaphragm alive” may be used to remember this relationship.) The acquired form can also be seen in older patients after surgical trauma to the phrenic nerve. It may also be associated with Werdnig-Hoffman syndrome (spinal muscle atrophy), in which the progressive and generalized loss of neurologic function leads to eventration. On surgical exploration, congenital and acquired forms can be distinguished because, whereas a congenital diaphragmatic eventration has a greatly thinned central portion of the affected diaphragm, an acquired diaphragmatic eventration (if operated on early) has a normal-appearing, but weakened, muscle.[3]
Treatment of diaphragmatic eventrations will vary, mostly according to the size of the eventration and the clinical status of the patient. Small eventrations can be left untreated, but large ones require repair, even when asymptomatic, in order to allow for proper lung development. Untreated diaphragmatic dysfunction causes a restrictive deficit, with reduced lung volumes, smaller tidal volumes, and increased work of breathing. Patients with respiratory distress need prompt attention and supportive care with endotracheal intubation and ventilation. Patients should not have oral intake. A nasogastric tube should be passed to decompress the stomach, and intravenous fluids should be initiated. Once the patient is stable, surgery is indicated. Repair can be done through the abdomen or the chest and, depending on the experience of the surgeon, the approach may be open or minimally invasive.[4] A thoracotomy or thoracoscopy is usually preferred, except when concomitant abdominal abnormalities, such as malrotation, are suspected. Multiple nonabsorbable sutures are utilized in a staggered fashion across the diaphragm to pull and flatten the muscle. This plication maximizes the intrathoracic space by imbricating the diaphragm to a near horizontal position. Generally, chest tubes are maintained for up to several days and rapid clinical improvement is observed; however, other techniques, such as evacuation of air while closing the intercostal space, have also been described.
The differential diagnosis of diaphragmatic eventration includes congenital diaphragmatic hernias (also known as Bochdalek hernias). These hernias occur most commonly on the left side (90%), and the diaphragm itself is not normally visualized in radiographic examinations (except when a thick hernial sac is present).[2,3] Diaphragmatic eventrations, however, can occur on either side of the chest, and patients are usually asymptomatic for longer periods of time because they lack the pulmonary hypoplasia associated with diaphragmatic hernias.[3] When a true hernia is present, fluoroscopic or ultrasonographic evaluation reveals paradoxical diaphragmatic movement caused by pressure changes during ventilation. Inspiration creates a higher negative intrathoracic pressure, which pulls the diaphragm upwards. It is important to distinguish between these 2 entities preoperatively, because most pediatric surgeons would approach a diaphragmatic hernia through the abdomen in order to concomitantly correct the ever-present malrotation associated with these hernias. Diaphragmatic eventration, however, is best approached through a low thoracotomy, which enables adequate plication of the diaphragm and excision of the pulmonary sequestration that is present in many of these patients.
The patient in this case was admitted to the hospital and was kept without any oral intake. Broad-spectrum antibiotics were started, and an orogastric tube was passed to decompress the stomach. Intravenous fluids were given at a maintenance rate, and supplemental oxygen was administered. Once the patient was stable, he was brought to the operating suite, and the thorax was approached (see Figures 3 and 4) through a right posterolateral muscle-spearing thoracotomy (muscle-spearing approaches diminish the incidence of postoperative scoliosis). The diaphragm was plicated with nonabsorbable sutures, without opening it (see Figures 5 and 6), and the chest was closed in a regular fashion. The patient recovered uneventfully. He was extubated in the operating room and resumed diet the same day. A chest tube was not inserted, as there was no lung injury during the procedure; instead, the pleural space was drained with suction during chest closure. The patient was discharged on postoperative day 2, without respiratory difficulty.
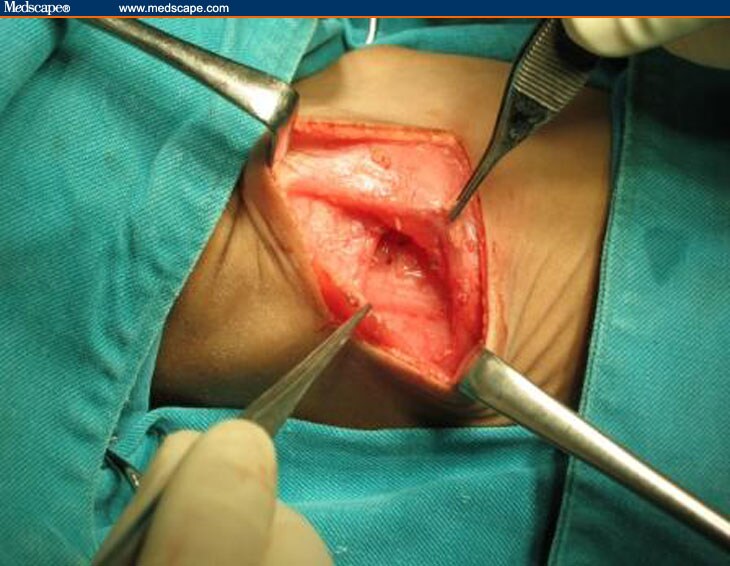 |
Figure 3. A right posterolateral muscle-spearing thoracotomy. (Click to enlarge) |
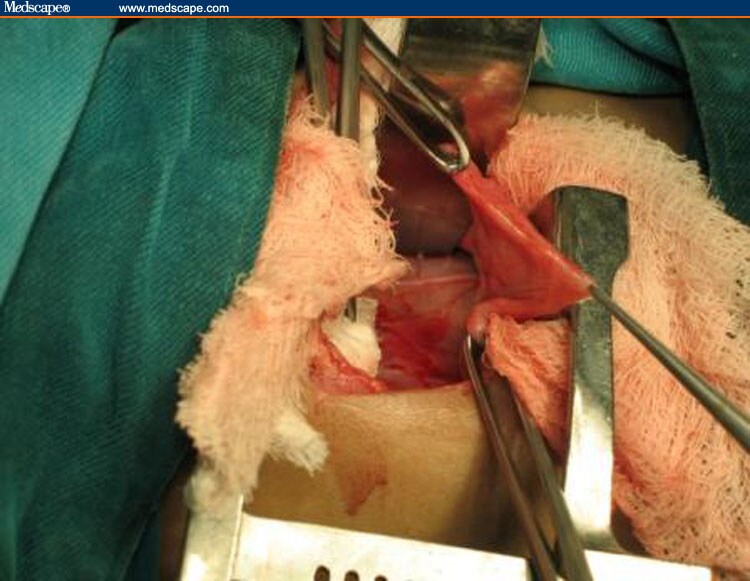 |
Figure 4. Weakened diaphragm. An elevated and weakened diaphragm seen during a thoracotomy. The phrenic nerve can be seen alongside the pericardium. (Click to enlarge) |
 |
Figure 5. (A and B): Sagittal scheme, diaphragmatic plication. (Click to enlarge) |
 |
Figure 6. Lung insufflation. Normal lung is seen properly insufflating after the diaphragm has been plicated. (Click to enlarge) |
At follow-up 6 months after surgery, the patient was doing well and was asymptomatic, as well as growing and gaining weight properly. There were no signs of respiratory difficulty or increased incidence of respiratory infections. The surgical wound had healed properly, and no scoliosis had developed. The follow-up chest radiograph revealed a partially flattened diaphragm (which is a normal postoperative finding), as well as complete lung expansion.
Tags: News




Leave a Reply
You must be logged in to post a comment.